Obesity Clinic in Colombia: Bariatric Surgery, Robotic & Medical Programs at Global Obesity Group

Obesity is a chronic disease, not a personal failure — and treating it requires the same scientific rigor used for diabetes or hypertension. At Global Obesity Group in Bogotá, we offer a complete continuum of evidence-based options: from gastric balloon and Da Vinci robotic bariatric surgery to Método 4 PRO, our non-surgical functional medicine program. International patients save 50–70% compared to U.S. private bariatric programs while receiving the same standards of care.
Plan your visit Meet your surgical team
Why Choose Colombia for Comprehensive Obesity Care
Colombia has become a recognized regional hub for bariatric and metabolic surgery. The country is an active IFSO-Latin America member, and the Colombian bariatric society (ACOCIB) certifies surgeons trained at the same fellowship programs used by ASMBS-accredited centers in the United States.
Bogotá in particular has concentrated expertise: three tier-1 hospitals — Clínica Shaio, Clínica Cobos, and Clínica Colsubsidio de la 100 — equipped with Da Vinci Xi robotic systems and full ICU support, all within 30 minutes of El Dorado International Airport.

The cost reality drives most international patients here. A primary gastric sleeve in the United States private market averages USD $15,000–25,000 when paying out-of-pocket. At Global Obesity Group the same procedure is USD $7,800 laparoscopic — same instrumentation (Stryker, Medtronic), same Joint Commission–style hospital standards, same fellowship-trained surgeons. The savings come from healthcare system structure, not from cutting corners.
For a broader explanation of what defines an obesity clinic and how to evaluate one, see our companion guide: Clinics for Obesity: A Complete Guide.
Understanding Obesity: A Chronic Disease, Not a Choice
The American Medical Association formally classified obesity as a chronic disease in 2013, aligning with the WHO and the National Institutes of Health. This matters clinically: obesity isn't a willpower problem, it's a multifactorial disorder of energy regulation involving hormones (leptin, ghrelin, GLP-1), gut microbiome, sleep, stress, genetics, and environment.
This is why long-term diets fail in roughly 80% of cases. The body defends a hormonal "set point" weight — after weight loss, ghrelin rises, leptin drops, and metabolic rate decreases, all pushing the body back toward its prior weight. Bariatric surgery and modern obesity medications work because they reset that hormonal signaling, not because they suppress hunger by force.
Untreated obesity raises the risk of type 2 diabetes, hypertension, sleep apnea, non-alcoholic fatty liver disease (NAFLD), cardiovascular disease, infertility, and several cancers. It also carries a substantial mental-health burden — depression, social stigma, and reduced quality of life are part of the clinical picture, not separate problems.
Bray GA et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocrine Reviews 2018. PMID 29518206
Comprehensive Services at Global Obesity Group
Our model is comprehensive, not procedure-first. Every patient begins with a virtual or in-person evaluation that maps medical history, BMI, comorbidities, and personal goals. Based on that, our multidisciplinary team recommends the right pathway — surgical, medical, endoscopic, or a combined program.
Bariatric Surgery Procedures
Bariatric revision surgery is also available for patients who had a prior failed procedure (regain, complications, or anatomical issues). Learn about revision →
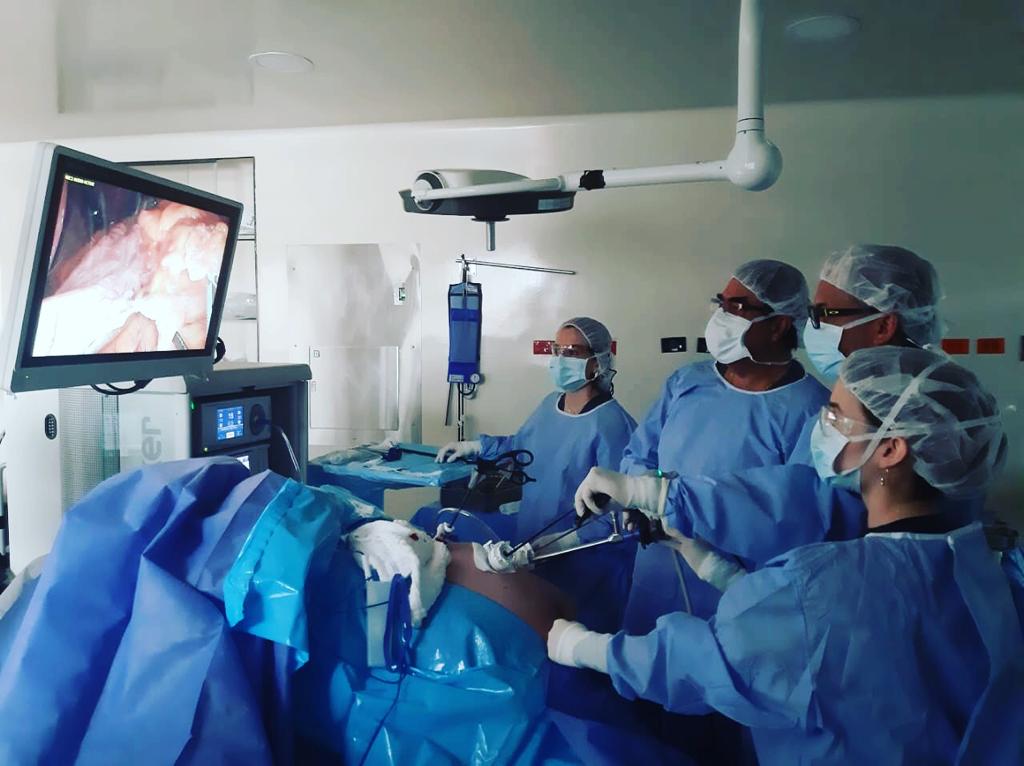
Da Vinci Robotic-Assisted Surgery
At GOG, robotic bariatric surgery is performed exclusively by Dr. Rubén Luna and Dr. Felipe Bernal, both trained on the Da Vinci Xi platform. The robotic approach uses three small incisions instead of the five-port standard laparoscopic technique, with sub-millimeter instrument articulation and 3D high-definition visualization. It is particularly valuable for high-BMI patients, complex revisions, and anatomically challenging cases.
Método 4 PRO (Non-Surgical Functional Medicine)
Created and led by Dra. Paola Sánchez, Director of Obesity Medicine at GOG, Método 4 PRO is a structured 12-month program built on four pillars: functional medicine and hormonal balance, clinical nutrition, health psychology, and physical activity. It is designed for patients who don't want surgery, don't yet meet surgical criteria, or who need to consolidate results after a procedure.
Método 4 PRO program details →
Multidisciplinary Support
Every track at GOG is supported by clinical nutrition, health psychology, and long-term follow-up. Functional medicine assessment is included for M4P patients and available as add-on for surgical patients. We use a minimum two-year follow-up window — standard in modern bariatric care — to track outcomes, address weight regain early, and adjust nutrition or behavior plans as needed.
Meet Your Medical Team
Our surgeons are certified by the Colombian Association of Bariatric and Metabolic Surgery (ACOCIB), members of IFSO and SAGES, and collectively have over 40 years of experience and 4,000+ bariatric cases performed.



See the full medical team and credentials →
The Science Behind Bariatric Surgery
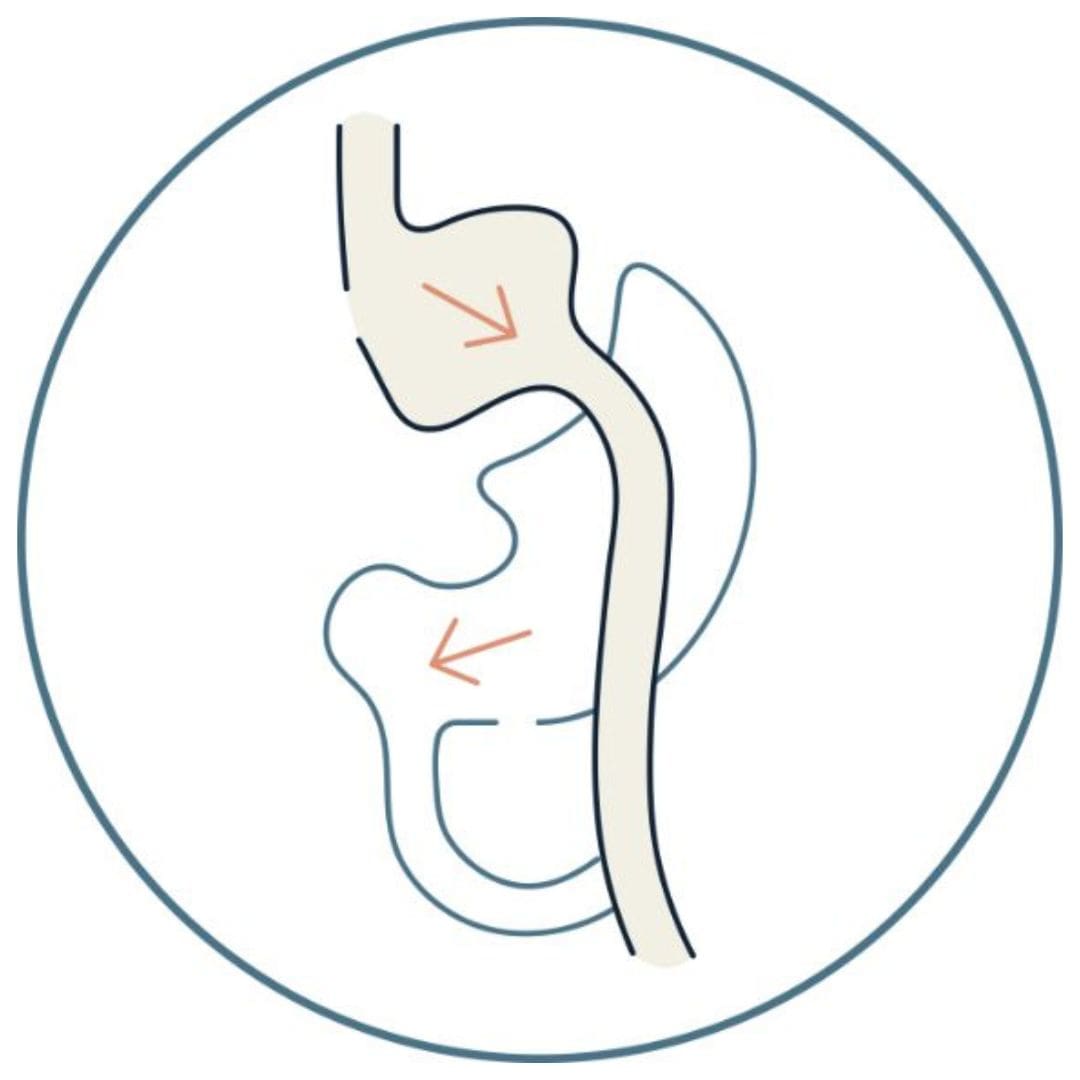
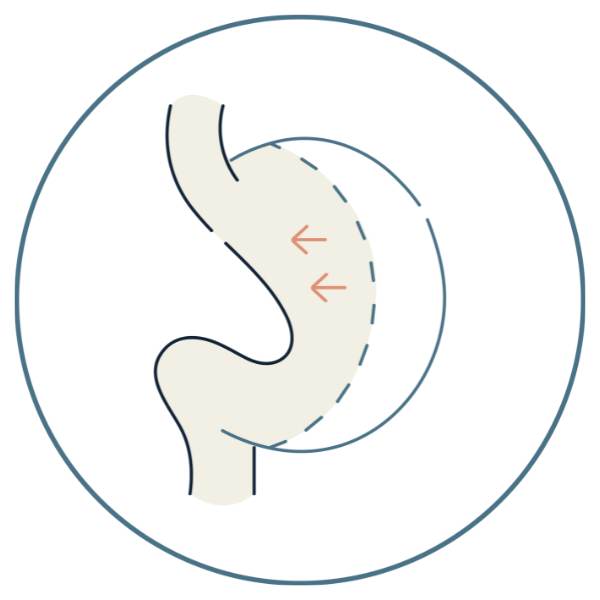
Bariatric procedures don't work by "shrinking the stomach to eat less." They work through two combined mechanisms. The mechanical change reduces stomach capacity and, in bypass, alters how food meets digestive enzymes. The neurohormonal shift is more powerful: post-surgery, the gut releases higher levels of GLP-1, PYY, and other satiety hormones, while ghrelin drops sharply. This is why patients describe a real loss of food obsession after surgery, not just smaller meals.
For type 2 diabetes specifically, the bypass produces neuroendocrine effects within days — often before significant weight loss occurs. The landmark STAMPEDE trial at 5 years showed bariatric surgery achieved sustained glycemic control in 29–23% of patients (sleeve / bypass) versus 5% with intensive medical therapy alone.
Schauer PR et al. Bariatric Surgery versus Intensive Medical Therapy for Diabetes — 5-Year Outcomes. N Engl J Med 2017. PMID 28199805
Gastric Sleeve vs Gastric Bypass: Which Is Right?
The right procedure depends on your BMI, your comorbidity profile, and your reflux history. The table below summarizes the practical differences. The final recommendation is a clinical decision made with your surgeon, not a checklist.
| Factor | Gastric Sleeve | Gastric Bypass |
|---|---|---|
| BMI range | 30–50 | 35+ (gold standard 40+) |
| Mechanism | Restrictive | Restrictive + malabsorptive |
| Avg. excess weight loss (1 yr) | 60–70% | 70–80% |
| Type 2 diabetes remission | 60–70% | 80–90% |
| GERD / reflux | Can worsen existing reflux | Often improves reflux |
| Reversibility | No | Partial |
| Hospital stay | 1 night | 1 night |
| Laparoscopic price (USD) | $7,800 | $7,800 |
| Da Vinci robotic price (USD) | $10,300 | $12,000 |
Laparoscopic vs Da Vinci Robotic: What's the Difference?
Both techniques are minimally invasive — small incisions, fast recovery, same hospital stay. The difference is the surgeon's interface and degree of precision.
Laparoscopic surgery uses five small ports and rigid instruments operated directly by the surgeon. It is the global standard for sleeve and bypass and produces excellent outcomes for most patients.
Da Vinci robotic surgery uses three ports. The surgeon operates from a console with two controllers; the robotic arms translate hand movements into instrument articulation with sub-millimeter accuracy. The surgeon sees a 3D high-definition view inside the abdomen rather than a 2D laparoscopic monitor. The robotic approach particularly benefits high-BMI patients (where abdominal wall thickness limits standard laparoscopy), complex revisions, and anatomically challenging cases.
The cost differential (roughly +$2,500–4,200 USD) reflects the Da Vinci platform fee and the higher cost of robotic disposable instruments — not a different level of surgeon. The same two surgeons at GOG (Luna and Bernal) perform both approaches.
Recovery & Post-Surgery Care
- Hospital stay: 1 night after sleeve or bypass.
- Recovery in Bogotá: 5–7 additional days before flying. We coordinate hotel accommodation for international patients during this window.
- Dietary phases: liquid (1–2 weeks) → puréed (2–3 weeks) → soft (3–4 weeks) → regular foods (8–10 weeks total).
- Activity: walking from day 1; no heavy lifting for 4–6 weeks; gradual return to exercise around week 6.
- Multidisciplinary follow-up: surgeon, clinical nutritionist, and health psychologist.
- International telemedicine follow-up: structured check-ins at 1, 3, 6, and 12 months post-op via video consultation.
- Long-term: minimum two-year follow-up program, in line with current ASMBS recommendations.
Benefits Beyond Weight Loss: Diabetes, Hypertension, and More
The strongest argument for bariatric surgery isn't aesthetic — it's metabolic. The most comprehensive long-term data comes from the Swedish Obese Subjects Study, which followed bariatric surgery patients for over 20 years and showed substantial reductions in cardiovascular events, type 2 diabetes incidence, and all-cause mortality compared with matched non-surgical controls.
- Type 2 diabetes remission: 60–90% depending on procedure.
- Hypertension resolution: ~50% of patients.
- Sleep apnea resolution: 60–80%.
- NAFLD / liver function: significant improvement in steatosis.
- PCOS and fertility: improved hormonal profile and conception rates.
- Joint pain (knees, hips): reduced loading and inflammation.
- Cardiovascular events and all-cause mortality: long-term reduction (SOS Study).
Sjöström L et al. Bariatric Surgery and Long-term Cardiovascular Events. JAMA 2012. PMID 22215166
Who Qualifies? BMI Categories & Eligibility
BMI is the standard starting point but it is not the only criterion. The presence of obesity-related comorbidities — type 2 diabetes, hypertension, sleep apnea, NAFLD — lowers the BMI threshold for surgical eligibility. Recent ASMBS/IFSO 2022 guidelines updated the indication for bariatric surgery down to BMI 30+ when significant comorbidities are present.
- BMI 27–30: gastric balloon or Método 4 PRO are typical first-line options.
- BMI 30–35: balloon, M4P, or sleeve depending on comorbidities.
- BMI 35–40 with comorbidities: bariatric surgery indicated (sleeve or bypass).
- BMI ≥ 40: bariatric surgery indicated regardless of comorbidities.
How to calculate BMI: BMI = weight (kg) / [height (m)]². Example: a person 1.70 m tall weighing 90 kg has a BMI of 31.1 — class I obesity.
Angrisani L et al. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes Surg 2018. PMID 30121858
Pricing: Transparent USD Costs
We publish pricing because international patients deserve clarity from the first email, not after a long sales process. All quoted prices include surgeon fees, anesthesia, hospital stay, post-operative medications, and one year of follow-up. Optional international concierge add-ons — airport pickup, hotel coordination, bilingual companion service — are quoted separately.
| Procedure | Laparoscopic (USD) | Da Vinci Robotic (USD) |
|---|---|---|
| Gastric Sleeve | $7,800 | $10,300 |
| Gastric Bypass | $7,800 | $12,000 |
| Bariatric Revision | $7,800 | $12,500 |
| Gastric Balloon | $5,000 | — |
| Método 4 PRO | Custom quote based on individual program | |
Need a personalized quote? Schedule your private virtual consultation →
International Patient Services
We've designed the international patient experience to minimize friction at every step. Bilingual coordinators (English/Spanish) handle scheduling, hospital coordination, and documentation. The pre-arrival virtual consultation is included in your package and helps confirm the right procedure before you book travel.
For the in-country stay, we assist with hotel recommendations near our partner hospitals — typically in the Chico and Usaquén neighborhoods of Bogotá, which are safe, English-friendly, and close to clinical facilities. Airport pickup and discharge transfer are part of the international package.
After you return home, post-operative follow-up is handled by video consultation in English at the standard 1, 3, 6, and 12-month checkpoints, with the option of additional appointments as needed.
Patient Outcomes: What to Expect
We report outcomes as ranges and averages drawn from peer-reviewed registries and our own patient pool, not as individual testimonial cases. Real before-and-after stories are published only with explicit patient consent and are intentionally limited.
Frequently Asked Questions
Is bariatric surgery in Colombia safe?
Yes, when performed by board-certified surgeons at accredited hospitals. Our surgeons are ACOCIB-certified, IFSO/SAGES members, and operate at tier-1 hospitals (Clínica Shaio, Clínica Cobos, Clínica Colsubsidio de la 100) using the same Da Vinci Xi and laparoscopic equipment used in the U.S.
How long do I need to stay in Bogotá?
Typically 7–9 days total: 1 night in the hospital plus 6–8 days for initial outpatient recovery before flying. The exact duration depends on the procedure and your individual recovery.
What hospitals does Global Obesity Group use?
Clínica Shaio, Clínica Cobos, and Clínica Colsubsidio de la 100 — all tier-1 institutions in Bogotá with Da Vinci robotic systems and full ICU support.
Does my U.S. insurance cover bariatric surgery abroad?
Most U.S. private plans don't cover overseas elective bariatric surgery. Some self-funded employer plans and medical-tourism specialty plans do — we recommend checking your policy directly. We provide itemized invoices to help with HSA/FSA reimbursement when applicable.
What's the difference between sleeve and bypass for me personally?
If you have type 2 diabetes, severe reflux, or BMI > 45, the bypass usually has the better long-term metabolic outcome. If you have a lower BMI, no diabetes, and no significant reflux, the sleeve is simpler with comparable weight loss. The final decision is made with your surgeon after evaluating your full profile.
Is Da Vinci robotic surgery worth the additional cost?
For most patients, standard laparoscopic surgery produces excellent outcomes. Robotic surgery adds meaningful benefit for high-BMI patients (thick abdominal wall), complex revisions, or anatomically challenging cases. Talk to your surgeon — sometimes the answer is laparoscopic, and that's the right answer.
What if I'm not ready for surgery? What are my options?
The Método 4 PRO program and the gastric balloon are both non-surgical pathways with strong outcomes for the right candidates. We never push surgery — the right decision is the one that fits your medical profile and life.
Who will be my surgeon?
You choose during your virtual consultation. The team includes Dr. Rubén Luna, Dr. Felipe Bernal, Dra. Carolina Rodríguez (bariatric surgery), and Dra. Paola Sánchez (obesity medicine, Método 4 PRO).
How fast can I schedule?
Most international patients schedule their procedure 4–8 weeks after their first virtual consultation. Required pre-op tests can usually be done in your home country.
Will I need follow-up after returning home?
Yes — and we provide it. Structured video-consultation check-ins at 1, 3, 6, and 12 months are part of your package. Additional appointments are available on request. Long-term follow-up beyond year one is also offered.
Ready to start your evaluation?
A short virtual consultation gives you a clear, personalized recommendation — sleeve, bypass, balloon, Método 4 PRO, or robotic surgery — and a transparent quote in USD.
- Bray GA et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocrine Reviews 2018. PMID 29518206
- Schauer PR et al. Bariatric Surgery versus Intensive Medical Therapy for Diabetes — 5-Year Outcomes. N Engl J Med 2017. PMID 28199805
- Sjöström L et al. Bariatric Surgery and Long-term Cardiovascular Events. JAMA 2012. PMID 22215166
- Angrisani L et al. IFSO Worldwide Survey 2016: Primary, Endoluminal, and Revisional Procedures. Obes Surg 2018. PMID 30121858